For a lot of people, weekly therapy is enough. It holds. But for some patients it doesn’t, and when that happens, the instinct is often to assume something went wrong. Usually, that’s not it. What’s happening is that the condition needs more than a single weekly hour can provide.
According to SAMHSA’s 2024 National Survey on Drug Use and Health, roughly 14.6 million U.S. adults had serious mental illness in 2024, defined as symptoms that substantially interfered with major life activities. That’s a large group of people who may need more than a standard outpatient schedule.
This article walks through what clinicians do when that’s the situation: how psychiatry gets brought in, how virtual care fills gaps, and what a higher-support plan looks like from the patient’s side.
Quick Answer Summary
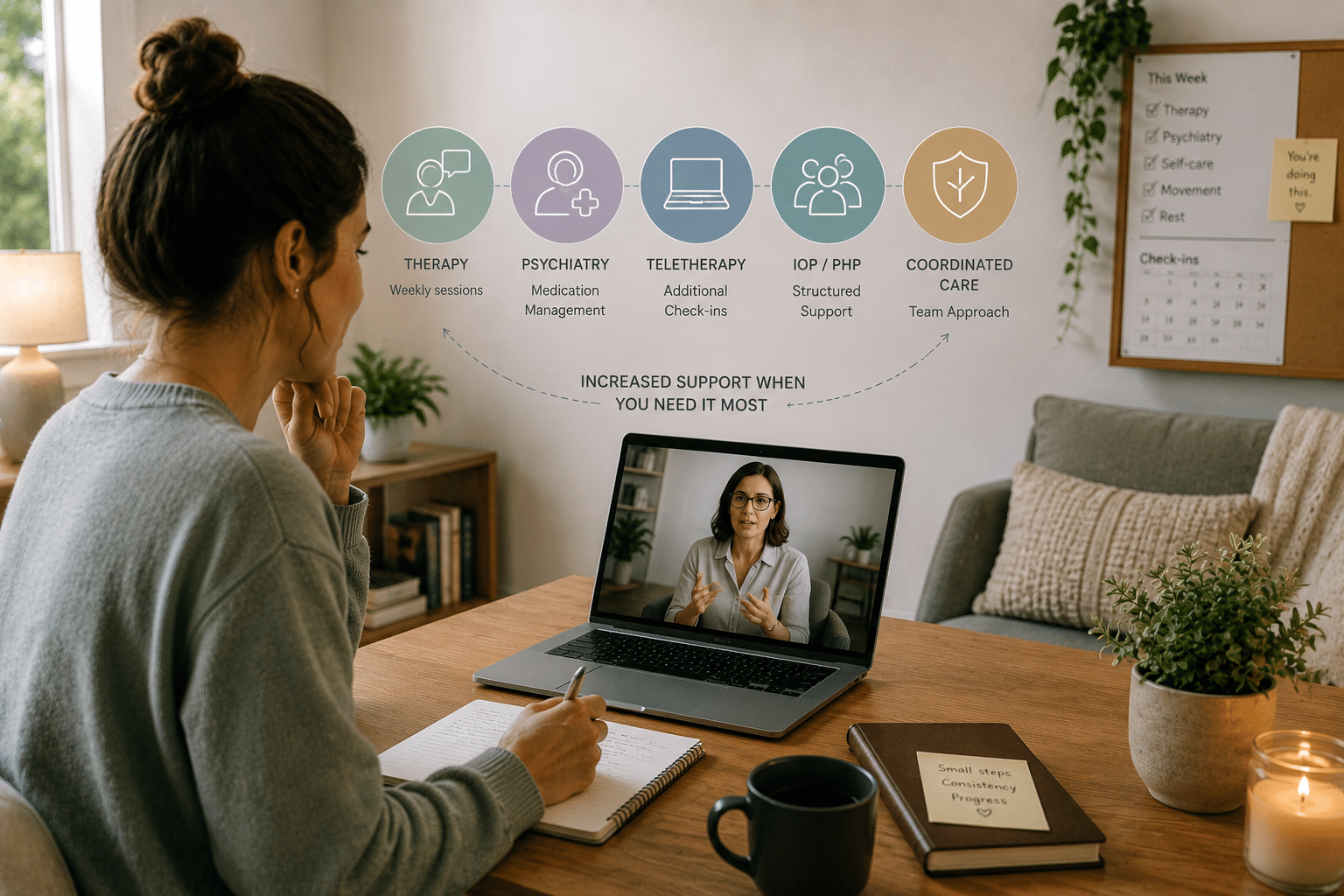
When therapy alone isn’t enough, clinicians add layers of support such as psychiatric care, medication management, more frequent sessions, teletherapy, or structured programs like IOP or PHP. These approaches provide additional stability, monitoring, and coordination to help patients manage more severe or persistent symptoms.
Key Takeaways
- Around 14.6 million U.S. adults have serious mental illness, often requiring more than standard weekly therapy.¹
- Signs that more support is needed include persistent symptoms, functional decline, and ongoing crisis-level stress.¹
- Psychiatry adds medication management, diagnostic review, and closer monitoring without replacing therapy.²
- Teletherapy helps increase access and frequency of care, with 48.3% of adults with serious mental illness using telehealth services.¹
- Digital tools and app-based interventions can reduce symptoms but are most effective as supplements to therapy.³
- Intensive Outpatient Programs (IOP) and Partial Hospitalization Programs (PHP) provide structured, higher-level care when weekly therapy isn’t enough.⁴
- Measurement-based care using tools like PHQ-9 and GAD-7 allows clinicians to track and adjust treatment in real time.³
- Coordinated care across therapists, psychiatrists, and providers improves stability and long-term outcomes.²
Signs That a Patient May Need More Than Therapy Alone
The shift doesn’t always announce itself clearly. Sometimes you’re several months into therapy before it becomes obvious the current structure isn’t working. Symptoms that should be getting better keep coming back. Sleep is still disrupted. Work is slipping. Relationships are straining. The patient is showing up to sessions, doing the work, and still not stabilizing.
That’s one version. Another is when sessions stop being about progress and become almost entirely about getting through the week. Crisis management instead of skill-building. And then there are safety concerns, including suicidal thoughts, self-harm urges, or anxiety so severe that day-to-day functioning isn’t safe.
Those aren’t signals to wait out. That kind of functional impairment, especially when it shows up across multiple life areas at once, is usually what prompts a clinician to reconsider the whole plan.
How Psychiatry Is Introduced or Expanded
Psychiatry doesn’t replace therapy. That’s probably the most important thing to understand upfront. What it does is add a different layer, like diagnostic review, medication evaluation, and closer monitoring of how symptoms are moving over time.
Medication gets added when therapy alone isn’t producing enough of a response, which is often the case with moderate-to-severe depression. For milder presentations, psychotherapy typically comes first.
When symptoms keep returning despite treatment, psychiatric treatment can look quite different. Treatment-resistant depression, typically defined as inadequate response to at least two antidepressants, may call for medication augmentation, esketamine, or TMS.
These aren’t early-stage options. They’re what gets considered when the more straightforward approaches haven’t worked. Psychiatrists also stay in contact with therapists during this process, because what happens in medication management and what happens in sessions need to stay aligned.
How Online Therapy and Teletherapy Supplement Care
Access is one of the biggest friction points in mental health care. Someone who needs check-ins twice a week instead of once faces twice the scheduling, twice the travel, twice the time off work. Teletherapy removes a meaningful chunk of that friction. It doesn’t fix every barrier, but for patients who need more frequent contact, it makes more contact possible.
According to the 2024 SAMHSA, 48.3% of adults with serious mental illness who received treatment did so via telehealth, about 7.1 million people. That number reflects how routine virtual care has become, especially for higher-acuity patients.
Online therapy also helps during transitions, like the gap between stepping down from an intensive program and returning to standard weekly sessions. That in-between period can be unstable, and virtual check-ins give patients something to hold onto. Digital tools like symptom trackers, CBT exercises, and mindfulness apps play a smaller supporting role.
In a 2024 Horwitz et al. trial, 2,079 adults in outpatient psychiatric care used app-based tools like CBT, mindfulness, or personalized feedback and saw depression and anxiety scores drop over six weeks. Useful, but only as a supplement. Therapy still does the heavy lifting. The apps just help patients stay in the work between appointments.
Moving Into Higher-Support, Structured Approaches
More frequent sessions is often the first move. Twice-weekly therapy, then a step back down once things stabilize. But there’s a range of patients for whom that still isn’t enough structure, and for them, Intensive Outpatient Programs (IOP) or Partial Hospitalization Programs (PHP) start to make sense.
IOP typically runs several hours a week and provides structured psychiatric treatment in a way that standard outpatient care can’t match. PHP is more intensive, at least 20 hours of services per week, and is usually for patients who need near-daily support but don’t require inpatient hospitalization.
There’s been a real policy recognition of how important these middle-ground options are. In 2024, CMS established Medicare coverage for IOP services after acknowledging the longstanding gap between weekly outpatient therapy and inpatient-level care. Clinicians at this stage may also add group sessions, skills-based formats, or family involvement, depending on what the patient needs.
Levels of Mental Health Support Beyond Weekly Therapy
| Level of Care | What It Includes | When It’s Used | Goal |
|---|---|---|---|
| Weekly Therapy | Individual sessions with a therapist | Mild to moderate symptoms | Build coping skills and emotional insight |
| Enhanced Outpatient Care | More frequent therapy + psychiatry + teletherapy check-ins | Symptoms persist or worsen | Stabilize symptoms with added support |
| Teletherapy & Digital Support | Virtual sessions, symptom tracking, CBT tools | Access barriers or need for more frequent contact | Maintain consistency and engagement |
| Intensive Outpatient Program (IOP) | Multiple sessions per week, group therapy, psychiatric care | Moderate to severe symptoms not improving with standard care | Provide structured, consistent support |
| Partial Hospitalization Program (PHP) | Daily treatment (20+ hours/week), full care team | High symptom severity without need for inpatient care | Stabilize and prevent hospitalization |
What Patients Can Expect From a Higher-Support Plan
More appointments is the obvious part. But the less obvious part is what happens between them. Regular symptom tracking with PHQ-9 for depression or GAD-7 for anxiety becomes routine. Clinicians use those numbers to adjust care in real time rather than relying only on how a session felt.
A 2025 JMIR study tracked 365,741 adults receiving therapy through a U.S. digital mental health provider across more than 2.6 million visits. Average PHQ-9 scores dropped from 9.41 at baseline to 6.37, and GAD-7 scores moved from 9.45 to 6.50. That’s what consistent, measurement-based psychiatric treatment can produce: gradual, trackable movement over time.
Patients also tend to find that care becomes more coordinated. A therapist, a psychiatrist, sometimes a primary care provider, all working from the same information. Safety planning may become a formal part of sessions when symptoms call for it.
Patients stay involved in the decisions throughout, and the step-up in care isn’t meant to be permanent. The structure is there to stabilize; the plan is always to step back down once things do.
When You Need More: A Stronger Safety Net
Needing more support isn’t a sign that treatment failed. It means the plan is adjusting to where the patient is, which is what good care is supposed to do. Sometimes that means bringing in psychiatry for medication management and closer follow-up. Sometimes it means adding teletherapy to stay connected between visits, or stepping into IOP when weekly sessions aren’t enough structure.
At Zeam, we approach it the same way. Our team in Sacramento, Folsom, and Roseville works together to match the level of support to what each patient genuinely needs. That might mean online therapy, medication management, TMS, Spravato, or a coordinated plan across multiple providers. If weekly therapy isn’t managing your symptoms, we want to help you figure out what will. Reach out today and let’s build the right level of care for where you are.
Citations
- SAMHSA NSDUH 2024 Annual Report:
https://www.samhsa.gov/data/sites/default/files/reports/rpt56287/2024-nsduh-annual-national/2024-nsduh-annual-national-html-071425-edited/2024-nsduh-annual-national.htm - Psychiatry & Treatment Escalation Context (JAMA Network Open):
https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2821341 - Digital Mental Health / JMIR Study:
https://www.jmir.org/2025/1/e75750 - CMS IOP Coverage Policy (2024):
https://www.cms.gov/newsroom/fact-sheets/cy-2024-medicare-hospital-outpatient-prospective-payment-system-ambulatory-surgical-center-payment