Ketamine therapy has moved from the edges of psychiatry into mainstream clinical practice, and for good reason. For people dealing with treatment-resistant depression, PTSD, or severe anxiety that hasn’t responded to standard medications, it can produce relief within hours rather than weeks. The evidence base is growing. The access points are expanding.
But the same qualities that make ketamine treatment powerful also make proper patient screening non-negotiable. This isn’t about gatekeeping; it’s about matching a specific treatment to a specific physiology and psychiatric profile.
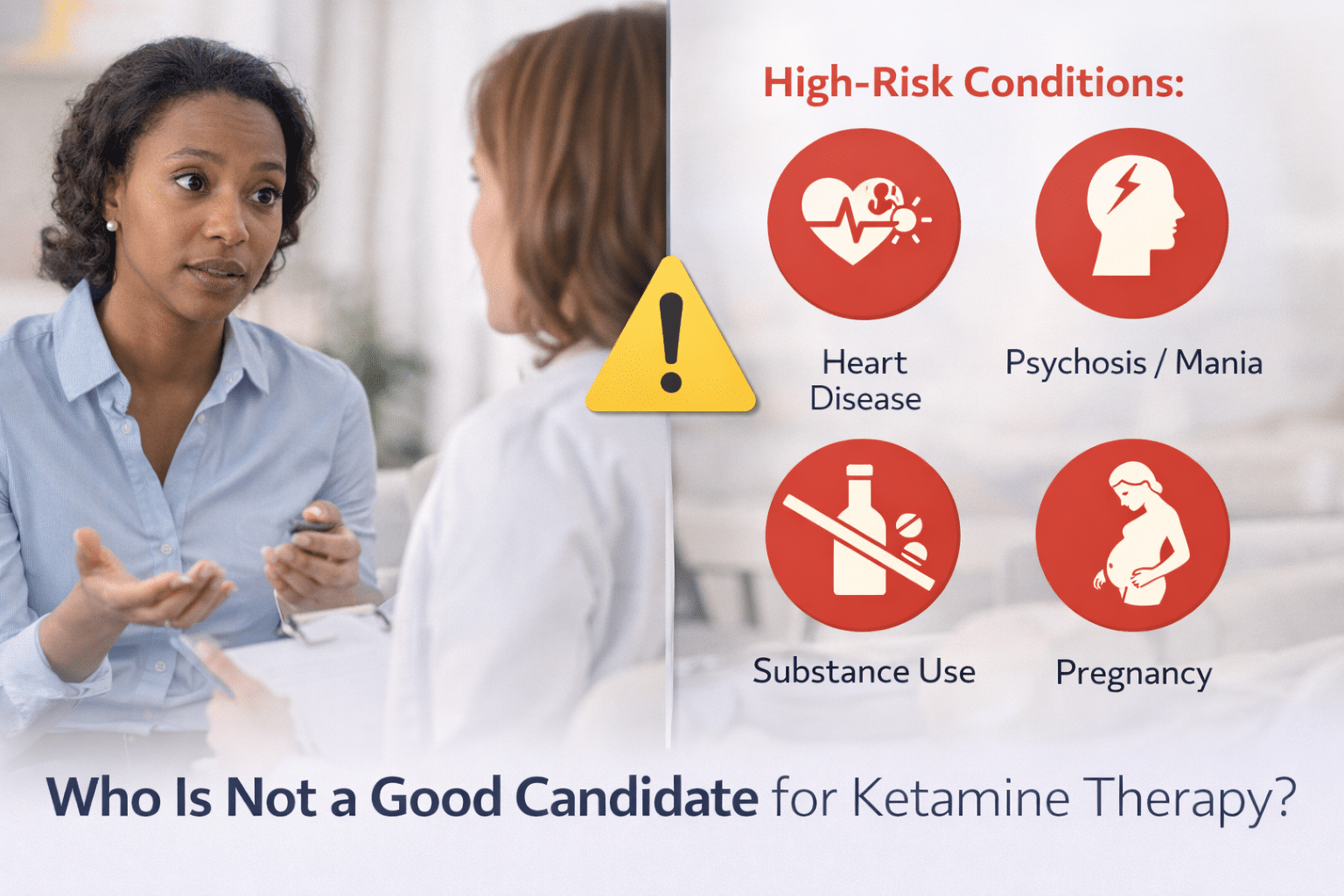
Some patients aren’t good candidates right now. Some aren’t good candidates at all. And the distinction between those two things matters.
Why Candidate Screening Exists in the First Place
Ketamine works differently from standard antidepressants. It targets the brain’s glutamate system, produces rapid neuroplastic effects, and causes transient dissociation and cardiovascular stimulation as part of its mechanism.
That cardiovascular stimulation, a sympathetic “kick” that raises blood pressure and heart rate, is expected, monitored, and managed in most healthy patients. In the wrong physiologic context, it becomes a problem.
The FDA’s Risk Evaluation and Mitigation Strategy (REMS) for Spravato (esketamine) requires that every treatment be administered in a certified clinical setting with at least two hours of post-dose monitoring. That structure exists specifically because the drug’s profile creates meaningful risk for certain populations. Understanding which populations means understanding the contraindications.
Cardiovascular Conditions That Create Real Risk
Cardiovascular health is arguably the most concrete category of concern with ketamine infusion therapy.
A retrospective chart review from Yale Psychiatry Hospital, covering 138 patients and 2,342 infusions, found that systolic blood pressure peaked at 40 minutes into the infusion, with a mean increase of 16 mmHg. Severe hypertension (defined as clinically significant elevations) occurred in 12.5% of patients across the study period.
Notably, every single patient with a prior history of hypertension experienced a blood pressure surge. Age also emerged as a significant independent predictor of blood pressure elevation.
Another clinical review found that 30% of analyzed participants experienced blood pressure exceeding 180/100 mmHg or a heart rate above 110 bpm at some point during infusion. In appropriately screened patients, these surges resolved within 2–4 hours without persistent cardiovascular events. The concern isn’t the spike itself but whether the cardiovascular system can safely absorb it.
Per FDA labeling for esketamine, ketamine therapy is formally contraindicated in people with uncontrolled hypertension, aneurysmal vascular disease, arteriovenous malformation (AVM), recent myocardial infarction, history of intracerebral hemorrhage, aortic dissection, and severe or unstable heart failure. Patients with controlled hypertension, blood pressure adequately managed below safe thresholds, face a different calculus and may proceed with additional monitoring.
Active Psychosis, Schizophrenia, and Unstable Psychiatric States
On the psychiatric side, ketamine’s dissociative properties that create therapeutic space for many patients can actively destabilize others.
The ASRA/AAPM/ASA consensus guidelines on IV ketamine infusions identify active psychosis and schizophrenia as contraindications, grounded in documented cases where subanesthetic ketamine reactivated hallucinations and delusions in people with schizophrenic disorders.
Research funded through the NIH’s Intramural Research Program at NIMH confirmed that individuals with current psychotic symptoms are routinely and appropriately excluded from ketamine trial protocols because of the documented association between ketamine treatment and increased psychotic symptoms in both healthy controls and schizophrenic patients during and after infusion.
The FDA-pivotal trials that earned esketamine its approval for treatment-resistant depression excluded patients with active psychosis and schizophrenia entirely. Professional societies have followed that lead.
Active mania also falls into this category. Ketamine’s dissociative effects can trigger manic cycling in people with bipolar disorder who are currently in a manic or hypomanic state. Bipolar disorder itself isn’t an automatic disqualifier. Researchers are actively studying ketamine therapy for depression in bipolar populations, but active mania at the time of treatment is considered an absolute reason to postpone.
Substance Use, Pregnancy, and Other Medical Factors
A few other categories require careful screening, though they’re often misunderstood as blanket disqualifiers.
Active, unmanaged substance use disorder is a relative contraindication for ketamine treatment options, according to the ASRA consensus guidelines. The concern is twofold: the abuse potential of ketamine itself (a Schedule III controlled substance), and the interaction between ketamine’s mood-lifting effects and an already dysregulated reward system.
A history of substance use doesn’t automatically disqualify someone. Timing, stability, and sustained recovery are what clinicians evaluate. Many programs require documentation of sobriety before proceeding.
Pregnancy and lactation are clearer. Ketamine is not recommended during pregnancy or when breastfeeding. Ketamine crosses the placenta, and the effects of repeated therapeutic exposure on a developing fetus are not established. Most U.S. clinics treat this as an absolute stop.
Severe hepatic impairment is a lesser-discussed factor. Ketamine is metabolized through the liver, so significantly impaired liver function can alter how the drug behaves and accumulates. This is typically evaluated on a case-by-case basis.
The Difference Between “Not Now” and “Not Ever”
It’s worth pausing here, because the list above can read like a wall of closed doors. It isn’t.
Absolute contraindications, like active psychosis, uncontrolled hypertension, aneurysmal vascular disease, pregnancy, and severe cardiovascular instability, are conditions where the risk to the patient is clear enough that treatment should not proceed regardless of how much someone wants relief. These are safety parameters drawn from FDA labeling, major clinical trials, and professional society consensus.
Relative contraindications are different. Controlled hypertension, stable bipolar depression, a history of psychosis that is currently well-managed, or documented recovery from substance use disorder require additional evaluation and monitoring, not automatic rejection. Many patients with relative contraindications move forward safely once their clinical team has the right information and puts appropriate precautions in place. What disqualifies someone today may not disqualify them in three months.
Self-screening is also an imprecise tool. People often assume they won’t qualify before anyone has evaluated them. A thorough clinical intake, one that includes medical history, psychiatric assessment, medication review, and vital sign screening, is what generates an accurate answer.
Screening Isn’t the End of the Road
Every year, more people find real relief through ketamine, but outcomes depend heavily on fit. Before any treatment begins at Zeam, our team works through a thorough medical and psychiatric evaluation to make sure the approach is right for you.
If you are in Sacramento, Folsom, or Roseville and have been uncertain about whether you qualify, or if a prior provider raised questions about your eligibility, we encourage you to reach out. The evaluation process is designed to give you a clear, honest picture of whether ketamine treatment options are a fit, and if they’re not, what alternatives might be.
Key Takeaways
- Ketamine therapy requires careful screening because it can cause transient dissociation and cardiovascular stimulation, including meaningful increases in blood pressure and heart rate.¹²
- Patients with uncontrolled hypertension, aneurysmal vascular disease, AVM, recent myocardial infarction, intracerebral hemorrhage, aortic dissection, or severe unstable heart failure are generally not appropriate candidates under FDA labeling.³
- A Yale retrospective review found ketamine infusions produced an average 16 mmHg systolic blood pressure increase, with severe hypertension occurring in 12.5% of patients.²
- Active psychosis, schizophrenia, and unstable mania are major psychiatric contraindications because ketamine’s dissociative effects can worsen hallucinations, delusions, or manic cycling.⁴
- Active, unmanaged substance use disorder is typically a relative contraindication, meaning timing, recovery stability, and clinical oversight matter more than history alone.⁴
- Pregnancy and lactation are generally treated as absolute reasons to avoid ketamine therapy, since fetal and infant exposure risks are not well established.³
- Severe hepatic impairment may also change whether ketamine is safe, since metabolism can be altered in patients with significant liver dysfunction.⁵
- Screening helps distinguish between “not now” and “not ever,” and many patients with relative contraindications may still qualify later with the right stabilization and monitoring.
Citations
- https://www.sciencedirect.com/science/article/abs/pii/S0163834324001555
- https://pmc.ncbi.nlm.nih.gov/articles/PMC10901779/
- https://www.accessdata.fda.gov/drugsatfda_docs/label/2025/211243s016lbl.pdf
- https://pmc.ncbi.nlm.nih.gov/articles/PMC6023575/
- https://pmc.ncbi.nlm.nih.gov/articles/PMC5859935/